
Colds and flus mysteriously disappeared over the past two years only to return recently in many countries, often with a vengeance. While only rarely discussed and frequently dismissed as a mere curiosity, the mystery of the disappearing flu is actually one of the most important events of the past two years. Unpacking this mystery provides deep insights into the future trajectory of the SARS-CoV-2 pandemic, exposes the abject failure of the vaccines to control the pandemic, and puts the final nail in the coffin on futile public health measures like masks and social distancing. Get ready for more than a few surprises as you follow me on another deep dive into Covid mayhem.
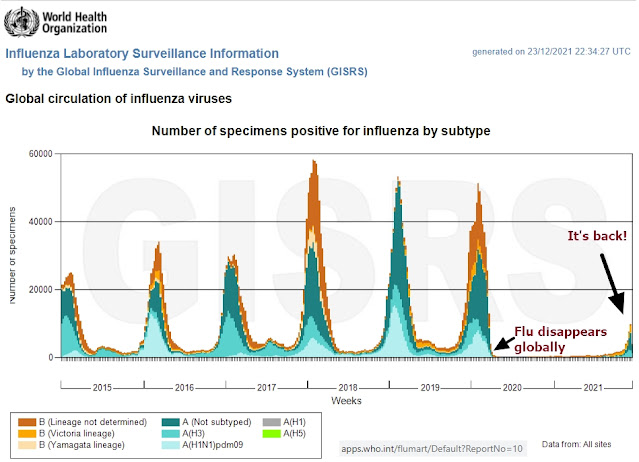 |
| Figure 1: Global circulation of Influenza viruses (Source: WHO FluNet) |
Table of Contents
- The Mystery of the Disappearing Flu
- Viral Interference: Why Did the Flu Disappear in the Early Days of Covid?
- New Virus, Same Role: Old Man's Friend
- Viral Interference Through Cross-Reactive Immunity - Only a Small Piece of the Puzzle
- Viral Interference Through Revving up the Immune System
- Underestimating How Many People Were Exposed to SARS-CoV-2
- We're Ba-ack! Important Lessons About the Return of the Flu (and Warnings for Countries Where the Flu is Still Missing)
- New Zealand: The Exception to the Rule
- India: The First to Achieve Broad Natural Immunity
- Brazil: The Flu Arrives Right on Schedule. Covid Becomes Endemic
- South Africa: Mild Omicron Can't Put the Flu Back in a Box
- Sweden: The Wisdom of Not Locking Down Proves Itself. Even Delta Had No Teeth
- Germany Proves Low Natural Immunity (Even with High Vaccination Rates) Is a Recipe for More Dying
- Canada: A Test Case for Omicron on a Population with Low Natural Immunity. Is Omicron Still Mild in a Population Without Antibodies?
- Kenya: A Pandemic So Mild That the Flu Never Went Away - Yet Another Embarrassment for Central Planning
The Mystery of the Disappearing Flu
Many public health officials and journalists credited masks, lockdowns, and social distancing for the disappearance of the flu. Critics pointed out that the flu also disappeared in places like Sweden, which did not have lockdowns, mask mandates, or social distancing rules. Critics also pointed to long-standing research demonstrating that virus-bearing aerosols are too small to be stopped by masks and that, even in perfectly still air, these aerosols are so small that they hang in the air for many days before settling to the ground, making social distancing a joke.
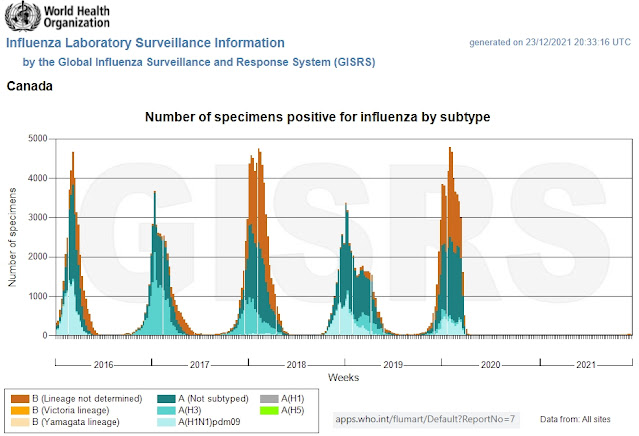
Particularly embarrassing for those cheerleading all these heavy-handed measures is that the flu disappeared several months before the first mask mandate was imposed, as demonstrated in the chart below showing influenza cases in Canada. I've added dates to the chart to show when mask recommendations and mask mandates were first rolled out — it's rather obvious that they had nothing whatsoever to do with why the flu disappeared. Clearly, we need to look elsewhere to explain the mystery of the disappearing flu.
 |
| Figure 2: Circulation of influenza viruses in Canada. The flu disappeared in Canada by March 30th, 2020. The first mask recommendation in Canada was made 2 months later on May 20th, 2020; prior to that date masks were actively discouraged by health officials. And the first mask mandate in Canada was imposed on July 18th, 2020, in the province of Quebec, four months after the disappearance of the flu. (Adapted from WHO FluNet) |
On the other side of the debate are some who have suggested that cold and flu infections were simply rebranded as Covid due to flawed PCR testing. However, in many countries flu testing did not stop, yet the number of flu tests coming back positive nonetheless fell off a cliff. Some countries even conducted more flu tests than usual and still found nothing. And cold and flu numbers also collapsed in countries like Japan, which had extremely low Covid infections during the early waves of the pandemic; they had low flu and low Covid numbers, so it was not a matter of shoddy accounting transferring cases from one balance sheet to another. The flu stopped circulating globally (I'll get to the surprising exceptions later in this article — hint: Kenya).
The chart below shows the total number of flu tests (on the left) and the percent of flu tests coming back positive (on the right) in Canada, the United States, and Europe. The dashed black lines show the pre-2020 averages in each region (grey shows the minimum and maximum number of tests in previous years). The red lines show the extraordinary 2020-2021 results: despite above-average flu testing in 2020-2021, flu cases essentially dropped to zero.
 |
| Figure 3: Number of influenza tests (left side) vs percent of tests coming up positive (right side) in Canada, the USA, and in Europe. During the 2020/21 season, the flu simply disappeared despite more testing than usual. From The National Influenza Annual Report, Canada, 2020-2021, published October 2021 |
In recent months a different phenomenon has emerged. Countless people all over the world are now complaining about brutal colds, which are NOT caused by Covid. The RSV virus has also returned. And the flu is back in many countries.
And these viruses are back with a vengeance, in some cases far above pre-2020 levels thanks to the immunity debt that has built up in the population because of a lack of regular exposure to these other respiratory viruses. For example, RSV infections are swamping many hospitals at unprecedented levels, often despite large numbers of positive Covid tests still being recorded in the same communities.
And, rather embarrassingly for the pro-mask, pro-social distancing crowd, these viruses are back despite the fact that most countries still have universal mask mandates and social distancing rules. Check mate.
Viral Interference: Why Did the Flu Disappear in the Early Days of Covid?
In order to understand the significance of the return of the flu and what it means for Covid, we first need to solve the mystery of why the flu disappeared in the first place.
There is a well-known but poorly understood concept in virology called viral interference (also known as viral displacement). Virus interference was first described in plants in 1929 where the yellow-mosaic tobacco virus did not replicate in plants already infected with the common mosaic virus. This phenomenon is not restricted to plants; it also happens with animal and human viruses. The essence of this concept is that an infection with one virus can temporarily prevent or partially suppress infection with another different virus. And it happens all the time.
The most spectacular examples happen during a pandemic when a new virus (or new variant), which is relatively unfamiliar to our immune systems, displaces all the usual endemic respiratory viruses that normally cause colds and flus, just like what happened to the flu during Covid.
But that's not the only place viral interference happens. It also happens between variants of the same virus, as we've witnessed with Covid variants, as new more contagious variants displace older variants causing them to disappear each in their turn, seemingly overnight. An infection with one blocks infection with another. The breakneck speed at which the Omicron variant is currently displacing the Delta variant in many countries is perfectly normal behaviour - it's what you would expect. It happened exactly the same way when Delta arrived, when Alpha arrived, and so on.
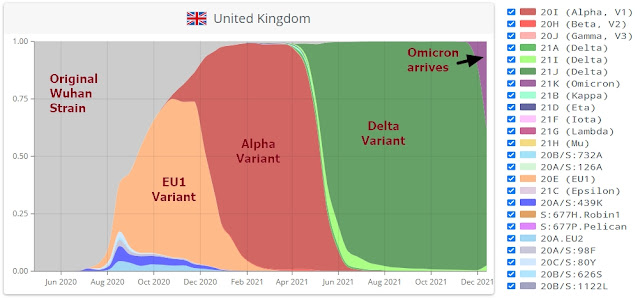 |
| Figure 4: Variants in the UK as a percentage of all Covid Cases. EU1 replaced the Wuhan strain, which was displaced by Alpha, which was displaced by Delta, and now Omicron is competing with Delta. Adapted from CoVariants.org. |
Viral interference also happens to a lesser degree during a normal year as all the other 200+ respiratory viruses compete to infect us — interference between them is why there generally are only a few that plague us at any one time. It's also why there is usually only a single dominant influenza strain each winter, not 3 or 4.
Viral interference also partly explains why different respiratory viruses have different seasons, rather than plaguing us all at the same time. For example, colds caused by rhinoviruses are much less frequent during influenza season:
 |
| Figure 5: Inverse correlation between rhinovirus cases and influenza A virus (IAV) cases. From Interference between rhinovirus and influenza A virus: a clinical data analysis and experimental infection study, The Lancet, October 1st, 2020. |
While environmental conditions certainly play a role in creating virus seasonality, viral interference ensures that there are usually only one or two dominant respiratory viruses at any one time. Once a large portion of a population is exposed to the dominant "virus of the day", that virus loses its ability to displace other viruses, thereby allowing another virus to step in and take its turn as the next "virus of the day", a kind of annual merry-go-round of alternating viral interference cycles.
The following graph shows how the seasonality of various respiratory infections is spread out over the year in England and Wales. It's as though each virus gets a slightly different time slot in the calendar, with some overlap but with clear alternating peak seasons, as though saturation with one virus opens the door to the next. Note how influenza viruses all cover an identical season: during influenza season the influenza virus suppresses other respiratory viruses, but the various flu strains (influenza A, B, C, and D) also compete with one another and the winner each season will displace the other influenza strains — this is why we typically only get one dominant flu strain each year. The annual flu shot is therefore an educated guess as to which flu strain is likely to displace the others each year. It also raises the question of how many severe illnesses and deaths the flu shot actually prevents if another virus will simply step into the void if a dominant strain is blocked through vaccination. After all, all of the endemic respiratory viruses that cause cold- and flu-like symptoms are a risk to the same vulnerable demographic: the old and the weak. Block one respiratory virus and another takes its place.
 |
Figure 6: Seasonality of Respiratory Viruses in England and Wales. Adapted from Coronavirus seasonality, respiratory infections and weather, BMC Infectious Diseases, October 26, 2021 |
New Virus, Same Role: Old Man's Friend
When the SARS-CoV-2 virus displaced influenza as the primary winter flu virus in 2020 (along with RSV and rhinoviruses to a lesser extent), Covid began harvesting the old and the weak just as influenza did every winter prior to 2020. This is not a flippant observation. Those who are at risk of severe outcomes from Covid are the exact same demographic that would normally be at risk of severe outcomes from infections with influenza, rhinoviruses, coronaviruses, parainfluenza, and so on. While some are more deadly than others, they are all essentially taking turns to threaten the same vulnerable population.
Any respiratory tract infection (viral or bacterial) that enters the lungs is called pneumonia. Pneumonia used to be nicknamed "old man's friend" because it often brought a fairly swift and painless end to a life that was already of poor quality and would otherwise have continued to decline. Old man's friend creates the winter peaks of deaths every year, taking those who are already on the threshold of death due to old age or severe underlying health conditions.
The chart below shows this ebb and flow of weekly all-cause mortality in Canada (Covid deaths are shown in purple). The past two years do not stand out from previous years despite the disappearance of the flu. The two winter Covid peaks are clearly within the same order of magnitude as previous bad flu seasons, very similar to the 2018/2019 or the 2015/2016 winter flu seasons. Covid displaced influenza and is now playing the role of "old man's friend".
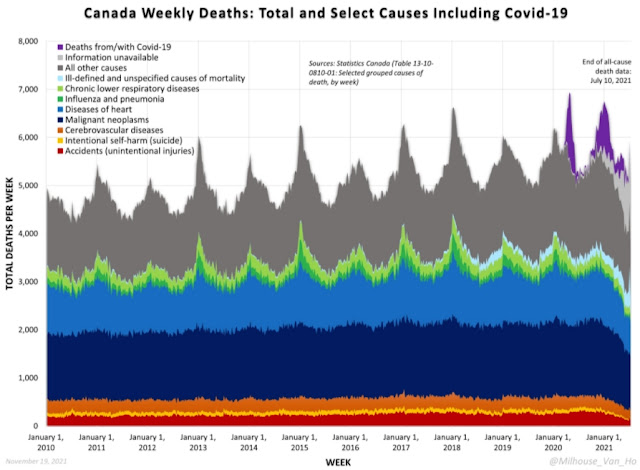 |
| Figure 7: 10 years of weekly all-cause mortality data in Canada. Covid deaths shown in purple show that the SARS-CoV-2 virus largely played the same role as "old man's friend" standing in for influenza during winter flu season. (Source: @Milhouse_Van_Ho) |
The raw Covid numbers (30,113 deaths in Canada as of December 22nd) would seem to contradict this. In a normal year between 6,000 and 8,000 people die of influenza or pneumonia in Canada, so we should only have seen approximately 14,000 Covid deaths during the pandemic if it were a true 1:1 replacement. But the higher Covid numbers are largely a product of PCR testing. Since Covid doesn't cure cancer or heart disease, the drops in heart disease, cancer, and other causes of death seen on the chart during the pandemic period are likely accounting errors caused by misattribution because any death with a positive PCR test was counted as a Covid death even if it was someone in a palliative care unit dying of cancer.
In 2018 no-one would have run a PCR test to look for influenza or rhinovirus or coronavirus in a long-term care patient dying of cancer, heart disease, dementia, or Alzheimer's, even if respiratory viruses did infect these patients as "old man's friend" in their final days of life. But in 2020 and 2021 that is precisely what is happening with Covid PCR tests, leading to a mass overcounting of Covid as the cause of death. Some Covid deaths really were caused by Covid, just as influenza and other respiratory viruses are the direct cause of some deaths every year, but Covid deaths were dramatically overinflated because of these misleading accounting practices.
However, what was unique over this period was that, because the SARS-CoV-2 virus was relatively unfamiliar to our immune systems compared to the regular respiratory viruses that normally plague us during cold and flu season, SARS-CoV-2 was able to hold on to its temporary monopoly as "old man's friend" for nearly 2 years, displacing other seasonal respiratory viruses that normally play that role.
And in case you think that Canada is an exception, the following chart shows weekly all-cause mortality in Europe since 2017. Covid shows up as two bad winter flu years, not as the apocalypse.
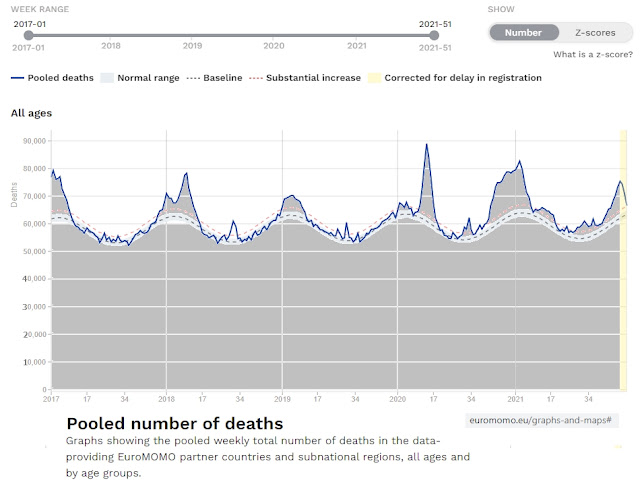 |
| Figure 8: All-cause mortality (in grey) in Europe, 2017-2021. X-axis has been extended to zero to show the winter peaks in context. Adapted from EuroMOMO (euromomo.eu) 2022. |
And when the flu returns, it will take over again as old man's friend during its slice of the annual merry-go-round of alternating viral interference cycles. Different viruses, same vulnerable population. The peaks and troughs on the charts above will continue even as the deaths are transferred out of the Covid column back to the columns where they belong.
Viral Interference Through Cross-Reactive Immunity - Only A Small Piece of the Puzzle
One of the factors that can cause viral interference between related viruses is when cross-reactive immunity from one virus carries over to another closely related virus lineage. Cross-reactive immunity explains why the dominant influenza variant can displace other influenza variants each winter or why new Covid variants are able displace older Covid variants.
With many people being infected by the SARS-CoV-2 virus, this triggered a surge of new antibodies, which likely also provided cross-reactive immunity to protect against the other four coronaviruses that normally cause 15-30% of all colds and flus each year. If these other four human coronaviruses were the only viruses that had disappeared during the pandemic, cross-reactive immunity would be able to take the credit. But cross-reactive immunity cannot explain the disappearance of influenza, rhinoviruses, and RSV. Why did they disappear too?
Viral Interference Through Revving up the Immune System
Remarkably, viral interference isn't just restricted to a single family of viruses. Even before Covid showed up it was well known that there is also viral interference between completely different viruses, such as between rhinoviruses (common cold) and influenza. This viral interference between unrelated viruses has everything to do with the different layers of our immune systems, which work in very different ways.
The cross-reactive immunity discussed in the previous section is a product of the adaptive immune system, which depends on previous exposure to teach the immune system how to recognize and combat future infections caused by a specific virus. Cross-reactive antibodies are a learned (trained) immune response. But those specialized antibodies cannot recognize and neutralize entirely different families of viruses.
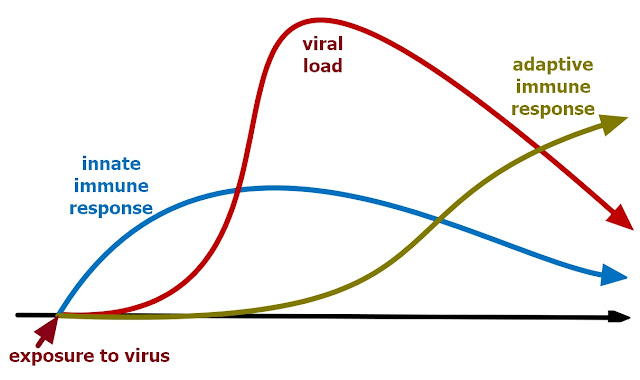 |
| Figure 9: Innate vs adaptive immune response. |
But this is where the other part of the immune system comes in: the innate (non-specific) mucosal immune system. The mucosal immune system is the largest component of our immune system. It has both an adaptive and an innate component - it is this innate component of non-specific antibodies that provides the key to the puzzle. Rather than relying on a specialized learned response, the innate mucosal immune system produces non-specific antibodies that attack and neutralize any invader that comes through the door - that's what makes it effective as a rapid response first responder. The innate mucosal immune system is not as powerful/specialized as the adaptive immune system, but it is the body's first line of defense against any germ that tries to creep up your nostrils. The much slower reacting adaptive immune system is designed to get involved as the innate non-specialized mucosal system gets increasingly overwhelmed. And here's where things get interesting...
An infection with a respiratory virus will trigger a massive temporary boost of the innate (non-specific) mucosal immune system. Our innate immune system is not static. In the process of fighting off one virus invader, our innate mucosal immune system is temporarily stimulated (revs up) to flood our upper respiratory tract with lots of these non-specific generalized "first responder" antibodies so that, for a brief time after infection, there is such an overabundance of these non-specific neutralizing antibodies that the mucosal immune system is able to temporarily ward off infections by many other viruses, thereby interrupting their transmission cycle in the population. In other words, the flood of non-specific antibodies released into the mucous membranes of the nose, mouth, nasal cavity, and throat to fight one infection primes the immune system so that for a short while afterwards there will be such an abundance of these antibodies ready to meet any a new virus that enters the upper respiratory tract that these subsequent intruders will immediately be zapped before they have a chance to replicate.
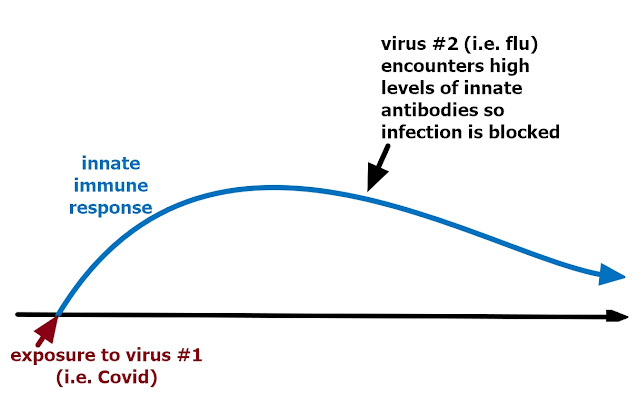 |
| Figure 10: Risk of an infection with another virus is lower while antibodies of the innate immune system are elevated. |
Another thing that happens during an infection is that infected cells will release signalling proteins called interferons (also called cytokines), first discovered in 1957, which send messages to surrounding cells to increase their innate anti-viral defenses. For example, rhinoviruses (common cold) trigger our innate immune system to release interferons that cause a subsequent infection with influenza to fizzle out. During the 2009 H1N1 Swine Flu pandemic, it is thought that the arrival of rhinovirus seasonality cut short the pandemic - the common cold cut short (displaced) the H1N1 influenza pandemic.
To what degree interferons are playing a role in causing viral displacement during Covid is uncertain. For example, contrary to what I just described in the previous paragraph, one type of interferon called IFN-I is actually suppressed or delayed by the SARS-CoV-2 virus (the opposite of what should happen), which is the reason why some people end up with severe Covid. In other words, the virus is actively fighting back against this portion of the innate immune system. However, there are many other types of interferon, and even a delayed interferon response would still help to block a post-Covid exposure to influenza, rhinovirus, RSV, etc.
And there is even some evidence that while a cell is infected with one virus, it blocks infection of that cell by another virus (a bit like a bathroom stall that is already occupied). In this case, it isn't even the immune system blocking other viruses, it is the fact that a virus that tries to enter an already occupied cell is unable to open the door to get in. This is one mechanism for how a virus can directly interrupt the transmission cycle of another virus, preventing simultaneous infections with two separate viruses.
While the phenomenon is well known, the exact mechanisms of viral interference are poorly understood - this is the fuzzy leading edge of science where there are more questions than answers. But when all these mechanisms are combined with a relatively unfamiliar virus (which triggers a particularly strong innate immune response because it is still relatively unfamiliar to the adaptive immune system) and when a very large number of people get infected within a short period of time (i.e. during a pandemic), you have the perfect recipe to interrupt the transmission cycle of all the other respiratory viruses, causing them to be displaced for a while.
Underestimating How Many People Were Exposed to SARS-CoV-2
Throughout the pandemic, our public health officials and media have kept everyone's eyeballs fixated on PCR "cases, cases, cases". While generating a lot of fear, this fixation on "cases" has actually kept everyone distracted from the results of antibody testing, which have consistently revealed that the virus was far far more widespread (and therefore also far less dangerous) than what PCR tests would have us believe. Orders of magnitude more widespread. More than enough to interrupt the transmission cycles of other respiratory viruses through viral interference.
Back in October of 2020 (only 7 months into the pandemic), the WHO estimated that there were already over 750 million SARS-CoV-2 infections (10% of the global population). But at that time PCR testing had only caught 36 million cases worldwide (0.46% of the global population). In other words, even if we disregard the massive false positive rates of PCR tests when testing asymptomatic people, PCR "case" numbers only accounted for approximately 5 percent of people who developed antibodies against the SARS-CoV-2 virus (both antibody tests and population-wide surveys done at blood donor clinics have all consistently confirmed that actual infections far exceed the number of "cases" recorded by PCR tests). And every one of those "infections" (exposure might be a more appropriate term) temporarily revved up the innate immune system, triggered the release of interferons, and blocked other respiratory viruses from infecting cells.
As an aside, to understand how quickly the SARS-CoV-2 virus can spread through a population without lockdowns, consider that 80% of Iowa's white-tailed deer were infected by the SARS-CoV-2 virus in a single winter in 2020/21, despite the fact that Iowa's woods are not filled with coughing, sneezing, or dead deer, and the deer are spread over vast outdoor distances. SARS-CoV-2 is everywhere.
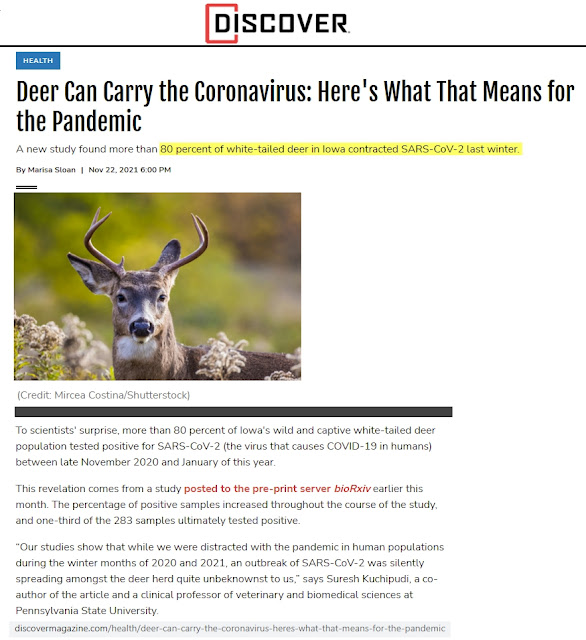 |
| Figure 11: 80% of white-tailed deer in Iowa contracted an infection with the SARS-CoV-2 virus last winter (Source: Discover, November 22, 2021) |
My point is that, even as PCR tests are being used to torment school children, lock up healthy people, and violate civil liberties, they also distract from the massive number of people who have actually already been infected/exposed and have developed antibodies without ever developing any symptoms. Exposure to the SARS-CoV-2 virus was far more widespread than many people realize, more than enough to rev up immune systems and temporarily break the transmission cycle of many other common respiratory viruses.
- The SARS-CoV-2 virus was far more widespread than "case" numbers would have us believe, more than enough to stimulate the innate mucosal immune systems of vast portions of the population, thereby temporarily blocking infections with other respiratory viruses and interrupting their transmission cycles.
- And because the SARS-CoV-2 virus was a relatively unfamiliar virus to our immune systems, it triggered a very strong immune response in our innate mucosal immune systems. Combined with a very large number of infections, this enabled SARS-CoV-2 to hang on to its role as the dominant virus for a very long time as it interrupted the normal annual merry-go-round of alternating viral interference cycles in other seasonal respiratory viruses for almost two full years.
- But — and this point is very important as we start to dig into the lessons offered by countries where the flu is returning — once our immune systems have some exposure to a new virus, our adaptive immune system will do more of the heavy lifting during subsequent re-infections, which means that our innate non-specific immune system will not be as strongly stimulated during future re-infections as during the initial exposure. When this tipping point happens, SARS-CoV-2 becomes just another virus, forced to compete for a time slot in the annual viral displacement merry-go-round. Unless it dies out altogether (unlikely), that's the moment it becomes an endemic virus, joining its four other coronavirus peers in causing colds and flus each season. Just another old man's friend. Thus, the return of the flu marks a pivotal tipping point in the evolving Covid pandemic. It is signalling a return to business as usual.
We're Ba-ack! Important Lessons About the Return of the Flu (and Warnings for Countries Where the Flu is Still Missing)
It's dangerous to apply a single explanation for complex phenomena happening in different parts of the world. New Zealand is the exception to the rule:
New Zealand - The Exception to the Rule
New Zealand essentially sealed off their island to the outside world during Covid and has consequently had very few SARS-CoV-2 infections to date. By April of 2021, Covid antibody testing in New Zealand showed that only about 0.1% of the population had been exposed.
With so few infections, viral interference likely only played a very small part in the disappearance of the flu. Instead, the temporary disappearance of other respiratory viruses likely had more to do with brutal domestic lockdowns and (more importantly) because, in a global world with constant travel between countries, closing borders and completely sealing out international travellers from their island caused an interruption in the normal inter-continental (or inter-island) transmission cycle of other respiratory viruses.
New Zealand has a population of 5 million. In a normal (non-Covid) year, an additional 1.6 million Australians visit New Zealand every year and over 1.4 million New Zealanders normally visit Australia each year. From a seasonal respiratory virus' point of view, Australia and New Zealand were effectively one country before Covid. Furthermore, prior to the pandemic over 3 million New Zealanders (two-thirds of their population) traveled abroad every single year and more than 11 million foreigners visited New Zealand from every corner of the globe every single year. So, sealing New Zealand's borders massively disrupted normal seasonal respiratory virus transmission cycles.
But after two years of isolation, many New Zealanders have an immunity debt through lack of regular exposure to these seasonal respiratory viruses (in other words, they haven't been exercising their immune systems). Young children in particular who had little or no previous exposure to other respiratory viruses are now more vulnerable to severe outcomes due to this immunity debt. So, after a 2 year hiatus, New Zealand is now beginning to pay the price for their Covid-Zero fantasy by facing increased vulnerability to all the other respiratory viruses, without actually having acquired any meaningful levels of immunity to Covid during this interim "pandemic" period. They haven't escaped Covid - they have yet to face it when they finally reopen their doors to the world.
As the chart below demonstrates, lockdowns and border closures in New Zealand squashed cases of RSV viruses in young children for all of 2020 (in yellow). But midway into 2021 (in red), the large immunity debt finally led to a catastrophe. When an RSV virus outbreak finally did occur, the virus found so many vulnerable young immune systems that it led to massive numbers of RSV hospitalizations in young children.
 |
| Figure 12: ICU discharges for children aged 0-4 in New Zealand with non-Covid respiratory tract infections, by year. 2015 to 2018 are shown as grey lines. 2019 is shown in blue. The almost complete absence of RSV cases in 2020 is shown in yellow. And 2021 is shown in red when RSV cases suddenly explode mid-way through the year. Adapted from: Respiratory syncytial virus: paying the immunity debt with interest, The Lancet, October 22nd, 2021. |
Meanwhile, the flu is still entirely absent in New Zealand:
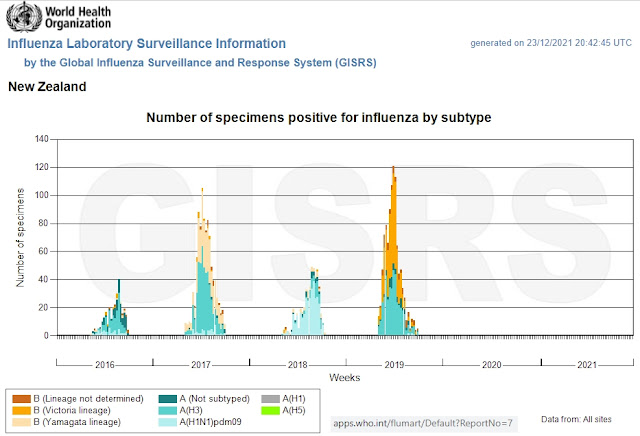 |
| Figure 13: Circulation of Influenza viruses in New Zealand (Source: WHO FluNet) |
In short, the disappearance of the flu and the reappearance of RSV virus in New Zealand are predominantly a product of self-imposed lockdowns and international isolation, while having little to do with viral displacement caused by the SARS-CoV-2 virus. Consequently, New Zealand's story has little to teach us about the future trajectory of the Covid pandemic in the rest of the world, though it should trigger massive outrage in New Zealand that their island has been subjected to misguided and authoritarian public health measures for two years, without actually leading to broad natural immunity against Covid. Talk about compounding mistakes, with interest!
By now it is obvious that the vaccines stop neither transmission nor spread. So, New Zealand's politicians have trapped themselves in a situation where, thanks to their complete self-imposed isolation, border re-openings will inevitably lead to a wave of infections and nursing home deaths, whether they are caused by Covid or by other returning respiratory viruses. Unlike other countries where Covid continued to play old man's friend in nursing homes, respiratory viruses have not taken their usual toll on New Zealand nursing homes for nearly two years so that once any respiratory virus (Covid or otherwise) gets into a New Zealand nursing home, it will find a particularly large vulnerable population, which will make for particularly frightening news headlines. Unless rational minds have the good sense to stop mass PCR testing of asymptomatic individuals in New Zealand and to educate their public that the vulnerability of nursing home patients does not mean that the rest of the population faces the same high level of risk, every attempt to reopen the border will lead to surges in respiratory virus outbreaks, waves of nursing home deaths, and trigger fresh panic.
But the return of the flu in countries like India, Brazil, South Africa, Sweden, and Canada, which were not completely closed off from the world and where Covid has raged, tells far more interesting stories with large implications for the future evolution of the Covid pandemic.
And then there is the curious case of Kenya where the flu never disappeared, which has yet another important lesson to teach the world about pandemic management.
India: The First to Achieve Broad Natural Immunity
The first country to see the return of the flu was India in August of 2021. The timing of the return of the flu is revealing.
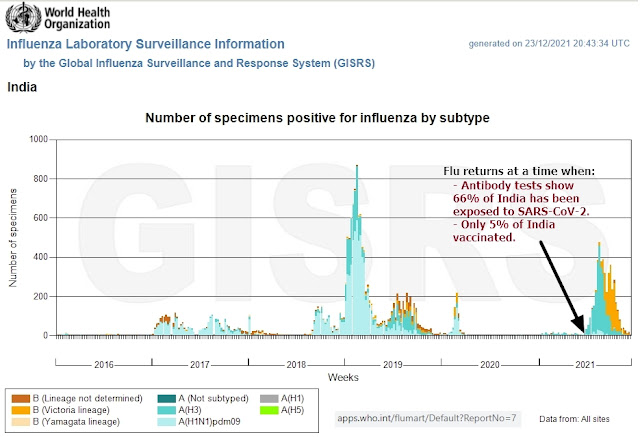 |
| Figure 14: Circulation of Influenza viruses in India. The flu returned at the point when 66% of India had antibodies to SARS-CoV-2 (despite only 5% of India having been vaccinated against Covid) (Source: WHO FluNet) |
Antibody tests in India showed that by June of 2021 over two thirds of their population already had antibodies even as vaccination levels were still under 5% (by November over 97% of people living in Delhi showed antibodies despite a vaccination rate of only 25%).
 |
| Figure 15: COVID cases in India (Adapted from World in Data) |
The return of the flu happened in India just after India completed a massive wave of Delta infections (long before mild Omicron came along). The return of the flu marks the tipping point when enough people acquired natural immunity to SARS-CoV-2 so that it stopped being able to displace other viruses. The return of the flu signals the end of the pandemic in India. Future variants of Covid are likely going to have to co-exist with all the other 200+ endemic respiratory viruses that cause colds and flus each year. The majority of immune systems in India have seen the SARS-CoV-2 virus at least once, so Covid ain't special anymore. Covid is now condemned to endemic mediocrity.
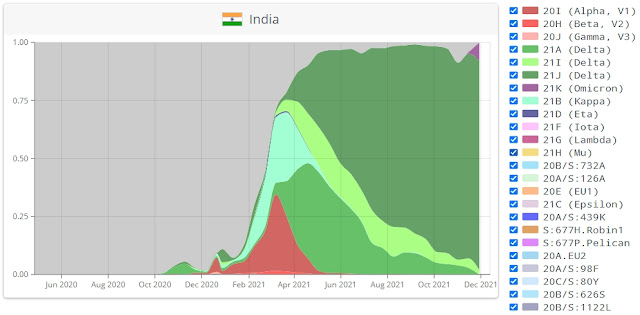 |
| Figure 16: Distribution of SARS-CoV-2 variants in India as a percentage of total SARS-CoV-2 infections. Original Wuhan strain in grey, Alpha variant in red, Delta in green, Omicron arriving in purple. From CoVariants.org. |
The timing matters because in India's case, the flu returned even before the milder (weaker) Omicron variant arrived. This confirms that in India's case the return of the flu is driven by its population having gained natural immunity to Covid, not by the mildness of the Omicron variant.
It is also worth noting that by the end of June of 2021, PCR tests had recorded approximately 30 million "cases" in India, whereas antibody testing showed that over two thirds of India's 1.38 billion citizens had already been infected - that's 910 million people. So, positive PCR tests only accounted for a mere 3.2% of all infections!
Brazil: The Flu Arrives Right on Schedule. Covid Becomes Endemic
By February of 2021, antibody testing in Brazil showed that up to 76% of their population already had antibodies for Covid in some regions of Brazil - this is BEFORE the vaccine rollout. Nonetheless, despite the high antibody levels, cases and deaths soared in the early part of 2021.
 |
| Figure 17: COVID deaths in Brazil (Adapted from World in Data) |
Despite the high level of natural immunity in some parts of Brazil in February of 2021, natural immunity was not yet universally distributed; it was still mostly constrained to pockets of the population (some cities). The large second wave in Brazil shown in the previous graph corresponds with the arrival of the Gamma variant in Brazil. The Gamma wave finally topped up the rest of the population with natural immunity (there is no free pass just because neighboring cities or provinces already achieved high natural immunity - the pandemic rages until the virus penetrates into every corner of a country). By the time the Delta variant arrived in July-August and displaced the Gamma variant, cases and deaths were in free-fall. The Delta wave's failure to re-ignite a fresh surge in cases and deaths demonstrates that the bulk of the Brazilian population achieved natural immunity to Covid during the Gamma wave, before Delta arrived.
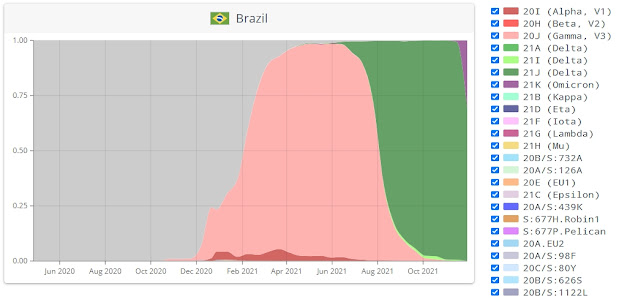 |
| Figure 18: Distribution of SARS-CoV-2 variants in Brazil as a percentage of total SARS-CoV-2 infections. Gamma variant in pink, Delta in green, Omicron arriving in purple. From CoVariants.org. |
 |
| Figure 19: Vaccinations in Brazil. Adapted from World in Data |
In December the flu re-emerged in Brazil, providing additional confirmation that the SARS-CoV-2 virus no longer has the ability to displace other respiratory viruses. SARS-CoV-2 has become familiar for most Brazilian immune systems. At this point, the Covid "pandemic" is likely also finished in Brazil.
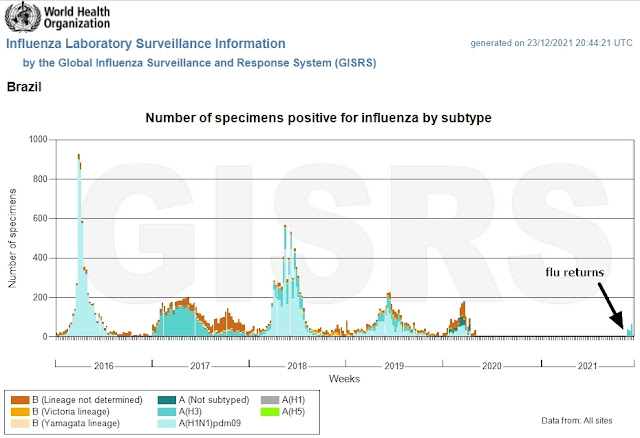 |
| Figure 20: Circulation of Influenza viruses in Brazil (Source: WHO FluNet) |
That doesn't mean Covid will disappear altogether. Future SARS-CoV-2 "variants" (like Omicron) will most likely simply behave as one of the 200+ respiratory viruses that compete for a slot in the rotating annual timetable of respiratory infections. If authorities keep up the dirty game of PCR testing, they will continue to find "cases". But they could do the same thing with literally any one of the other 200+ other respiratory viruses if they conducted mass PCR tests for those. Yawn. The best thing Brazil (and India) can do before Omicron arrives is to stop mass PCR testing to avoid triggering another unnecessary wave of panic.
South Africa: Mild Omicron Can't Put the Flu Back in a Box
Influenza is also back with a vengeance in South Africa, despite the fact that it is not normally influenza season at this time of year. An out-of-season arrival of the flu signals that viral interference from Covid has ended, allowing other viruses to come back even before seasonal environmental conditions are ideal.
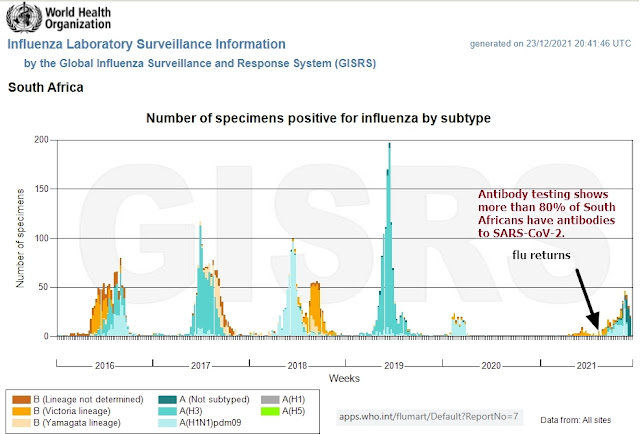 |
| Figure 21: Circulation of Influenza viruses in South Africa. Note that the flu is out-of-season. (Source: WHO FluNet) |
But what is unexpected in South Africa is that the flu is co-existing with SARS-CoV-2 (Omicron). Neither has displaced the other. They are competing.
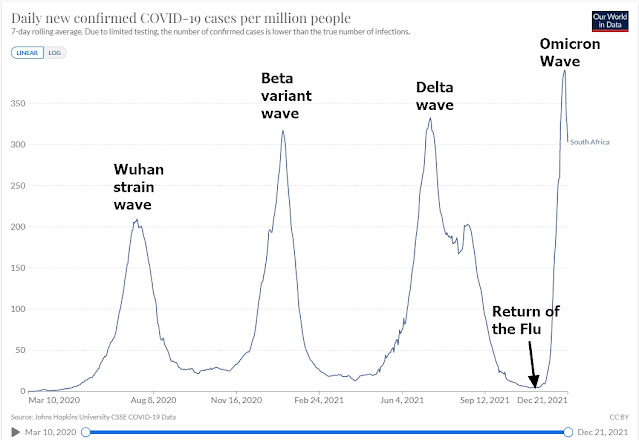 |
| Figure 22: Covid cases (via PCR test) in South Africa (Adapted from World in Data) |
Notice how each surge in Covid cases in South Africa corresponds with a different variant: the original Wuhan strain, the Beta variant, the Delta variant, and now the Omicron variant. Four separate pandemics, each variant displacing the previous one.
 |
| Figure 23: Variants in South Africa. Omicron (in purple) arrived around November 21 (corresponding with the surge in cases) and has completely displaced Delta. From CoVariants.org. |
But unlike previous surges of Covid, during the Omicron wave hospitalizations and deaths are not spiking in unison with Omicron infections. This makes sense because antibody testing in South Africa showed that by August of 2021 over 80% of their population already had antibodies to SARS-CoV-2 despite less than 6% being fully vaccinated at that time. The re-emergence of the flu in South Africa and its co-existence with Covid suggests Covid is no longer a novelty to South African immune systems, but it also suggests that, like other respiratory viruses, natural immunity won't cause Covid to disappear altogether.
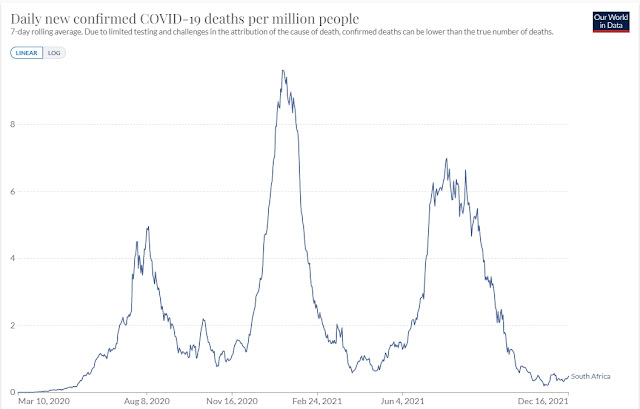 |
| Figure 24: Covid deaths in South Africa, with peaks corresponding to the original Wuhan strain in August of 2020, the Beta strain in December of 2020, and the Delta strain in August of 2021. So far, Omicron has failed to bring a new surge in deaths despite rising cases. (World in Data) |
In other words, South Africa provides the first piece of evidence that the SARS-CoV-2 is destined to become one of the other 200+ endemic respiratory viruses, rather than going extinct, because natural immunity provides partial protection against severe outcomes from future variants but does not block re-infection entirely. In other words, Covid is behaving just like any of the other colds and flus that plague us each winter. Until the day you die, no cold or flu will ever be your last. They are inconvenient but not life-threatening unless you have severe pre-existing health conditions or live in a nursing home.
Also worth noting is that, like during pre-Covid cold and flu seasons, there appears to be some overlap between coronavirus and influenza season, with Omicron following on the heels of influenza in South Africa. It may take a little while for all the normal seasonal respiratory viruses to settle into a regular routine again after such a large disturbance to seasonality, but normality appears to be returning to the South African respiratory virus scene.
The outstanding question is whether Omicron is mild because of high immunity in South Africa (in the same way that Delta was mild in Brazil because of high immunity even as Delta was still more severe in countries with low immunity), or whether Omicron is mild because it is a milder variant everywhere, regardless of pre-existing natural immunity. To answer that question, we'll need to look at Canada, which we will do momentarily.
Incidentally, as of December 23rd, PCR tests recorded a mere 3.4 million "cases" of Covid in South Africa, yet since 80% of South Africa's 59.31 million citizens already have antibodies, PCR tests only account for approximately 5.7% of all "infections". Conducting PCR testing and rapid antigen tests on asymptomatic people truly is a meaningless exercise... unless you want to instill fear and enrich testing companies.
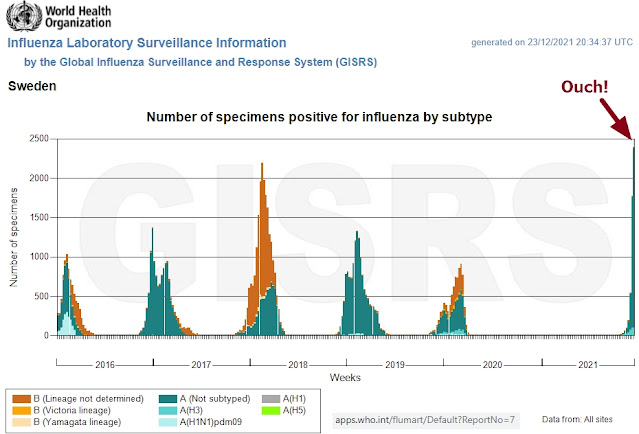
Sweden: The Wisdom of Not Locking Down Proves Itself. Even Delta Had No Teeth
Sweden never imposed any lockdowns, so the virus was as free to spread in Sweden as among Iowa's white-tailed deer population. Instead, Sweden followed the WHO's 2019 pandemic planning guideline, which every other Western nation ignored. And so, it should surprise no-one that the flu returned to Sweden long before any other Western nation. After such a long absence, the immunity debt to flu is causing a particularly large influenza season.
 |
| Figure 25: Circulation of Influenza viruses in Sweden (Source: WHO FluNet) |
Like in South Africa, Covid cases are also rising again this winter in Sweden:
 |
| Figure 26: Covid cases in Sweden. (World in Data) |
However, mild Omicron hasn't yet displaced the Delta variant - Sweden's current wave is still mostly being caused by Delta. Omicron has only just arrived.
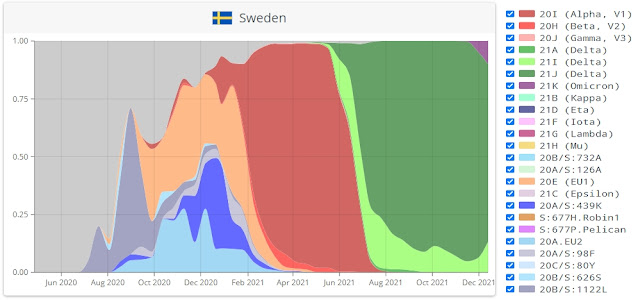 |
| Figure 27: Variants in Sweden. Most cases are currently from the Delta (green) variant. Omicron just barely has a toe in the door. From CoVariants.org. |
And yet, deaths in Sweden have remained flat since late February of 2021, before vaccination even began. There was no reason to vaccinate anyone in Sweden - Sweden ended its pandemic with natural immunity before vaccination began.
 |
| Figure 28: Covid deaths in Sweden. (World in Data) |
 |
| Figure 29: Vaccinations in Sweden. Adapted from World in Data |
The return of the flu alongside Covid and the absence of deaths despite rising Delta cases confirms that the pandemic is finished in Sweden. Solved by natural immunity. Even the Delta variant is behaving much like a mild endemic coronavirus that is now competing with the rest of the respiratory virus smorgasbord.
Sweden demonstrates that even large numbers of infections with the Delta variant do not pose a threat to countries with high natural immunity. High natural immunity in Sweden turned Delta into a toothless virus, just like in Brazil. There is no reason to think Omicron pose a threat once it arrives. The pandemic is over in Sweden.
And one more thing... a fresh wave of Delta infections in Sweden (despite basically everyone having natural immunity) means that many of the current infections in Sweden are re-infections in people who already have antibodies from a prior exposure. In a population with such high natural immunity, if natural immunity to SARS-CoV-2 provided sterilizing immunity, the virus would not find enough people to infect and would not be able to spread as easily as it is currently spreading (the herd immunity concept). So, as I explained in my previous deep dive, unlike viruses like measles whose spread is limited by high levels of sterilizing natural immunity, in the case of most common respiratory viruses (like colds, flus, and Covid) high levels of non-sterilizing natural immunity will not prevent future infections. Instead, natural immunity to these viruses prevents serious outcomes thanks to the partial protection to new variants provided by cross-reactive immunity. It's high time our public health officials stopped panicking about positive PCR tests and reminded its frightened citizens of how we have survived the annual return of cold and flu season every year since the dawn of time. Re-infection is the norm. Severe outcomes are not.
Germany Proves Low Natural Immunity (Even with High Vaccination Rates) Is a Recipe for More Dying
By contrast, Sweden's close neighbor Germany did go down the lockdown path and consequently still has a very low level of natural immunity in its population (as of November 24th, 2021) despite being over 70% vaccinated as of December 24th, 2021. Like in Sweden, Omicron has yet to get a proper toehold. Most infections during the current wave are from the Delta variant.
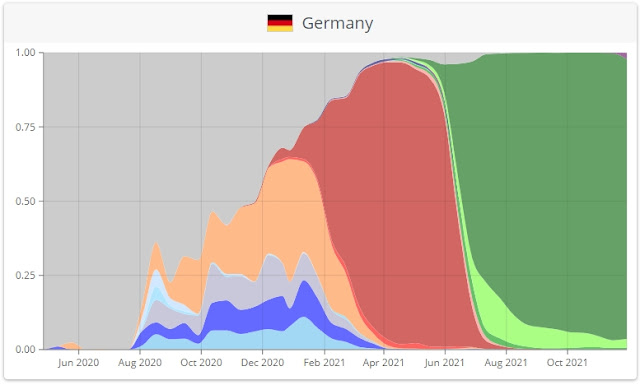 |
| Figure 30: Variants in Germany. Most cases are currently from the Delta (green) variant. Omicron just barely has a toe in the door. From CoVariants.org. |
However, unlike Sweden, the current surge in Delta infections in Germany is accompanied by a fresh wave in deaths. Not as bad as last year on the same date, but close. The low levels of natural immunity in Germany mean that, unlike Sweden, India, and Brazil, in Germany the Delta variant still has teeth. High vaccination rates have not stopped the dying in Germany, while high natural immunity in Sweden has. Same variant, different outcome, with the only difference between these countries being the high level of natural immunity in Sweden. Vaccination achieved nothing.
 |
| Figure 31: Covid deaths in Germany. (World in Data) |
Lockdowns in Germany prolonged the pain, violated civil liberties, destroyed economies, triggered inflation, and caused immense psychological suffering without making a measurable difference to deaths. The dying in Germany continues. By contrast, in Sweden, which avoided all these heavy-handed measures, the dying has stopped (Sweden had 1,494 deaths per million and the pandemic is over, while Germany currently stands at 1,314 deaths per million, but the dying continues and the pandemic continues to rage).
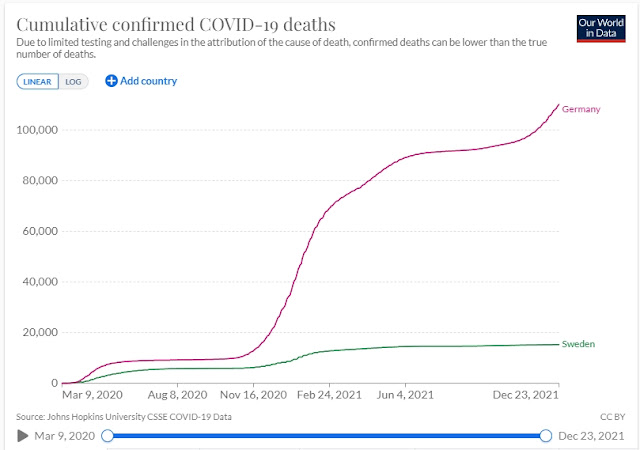 |
| Figure 32: Cumulative Covid deaths in Germany vs Sweden. High natural immunity in Sweden put a stop to the dying, whereas in low natural immunity Germany, the dying continues. (World in Data) |
Lockdowns slowed natural immunity and therefore prevented Germany's Delta wave from behaving as a nothingburger. The very same Delta variant that became a toothless tiger in high immunity countries like Sweden, India, and Brazil, is still causing deaths in a low natural immunity country like Germany, despite their high vaccination rate.
Natural immunity reduces deaths. Vaccination does not. The side-by-side example of Sweden vs Germany is the nail in the coffin for the Covid vaccines. And it is the most damning condemnation of our public health authorities who, quite literally, blocked what works (allowing people to lead normal lives) in order to impose a rushed and unproven vaccine experiment on society that does bugger all.
Oh, and the flu is still nowhere to be seen in Germany. Despite high vaccination rates, Germany's low natural immunity has not triggered a return of the flu because Covid is still raging among a population whose immune systems are still unfamiliar with Covid.
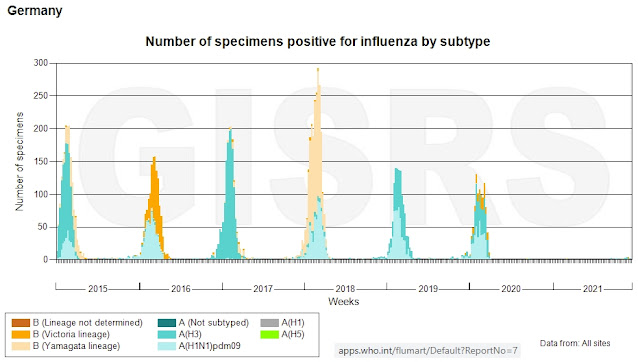 |
| Figure 33: Circulation of influenza viruses in Germany. The flu is still missing. (Source: WHO FluNet) |
The flu has already returned to some (but not all) of Canada's southern neighbors. In places like Florida, Wisconsin, Montana, and Pennsylvania where the flu has returned, the pandemic is likely finished, just like in Sweden.
Canada is not so lucky. It did everything it could to prevent the virus from spreading by imposing strict lockdowns and border closures. New Zealand lite. In all provinces. So, like Germany, it still has very low antibody levels; at the start of the vaccination campaign in January/February of 2021, a meagre 2.5% to 4% of Canadians had antibodies against Covid reflecting Canada's harsh rules. That number will be much higher by now, so Canada is not quite in New Zealand's island situation - the virus is here and circulating - but considering how strict Canada's authoritarian lockdown regime has been it is also unlikely that Canadian antibody levels are anywhere near levels seen in South Africa, Brazil, Sweden, or Florida.
And, as you would expect with such low natural immunity to Covid, the flu is still missing.
 |
| Figure 34: Circulation of influenza viruses in Canada (Source: WHO FluNet) |
Like in Germany, Sweden, and South Africa, cases in Canada are skyrocketing (despite Canada having a 77% vaccination rate !). However, unlike Germany, in Canada cases are being driven by the Omicron variant. Ontario's Chief Medical Officer has confirmed that a full 87% of all cases are now Omicron. Delta has been displaced by Omicron. And that makes Canada an interesting case study to test what happens when Omicron meets a population with low natural immunity but high vaccination rates (the exact opposite of South Africa's population). It is a repeat experiment of what is going on in Germany, with the only difference being that infections in Canada are being driven by Omicron rather than the Delta variant.
 |
| Figure 35: Covid cases (via PCR test) in Canada (World in Data) |
And the good news is that, unlike Germany, the SARS-CoV-2 virus appears to be losing its bite here too. Despite low levels of natural immunity in Canada, deaths are NOT surging in tandem with cases. Deaths are still flat. Omicron is mild. Omicron is toothless even in a population without high natural immunity.
 |
| Figure 36: Covid deaths in Canada (World in Data) |
Despite the fact that PCR case numbers during Omicron already outnumber cases during any of the other previous surges, so far hospitalization rates in Canada essentially haven't budged. They are slightly higher than during the Delta wave, which is to be expected since Delta arrived out of season (coronaviruses tend to flourish in mid-winter), so the hospitalization numbers during Omicron are extraordinarily low for a winter flu season. If it wasn't for all the PCR tests and rapid antigen tests, no-one would know there's a pandemic going on. Omicron is proving to be extraordinarily mild. I would bet that unless the flu returns, this may turn out to be the mildest winter flu season in Canada in decades.
The following graph shows the hospitalization rates in the province of Quebec. Omicron is hospitalizing more people than Delta but is still very very low for this time of year. For context, the current rate (Dec. 22nd, 2021) of 473 hospitalizations (in the entire province of Quebec!) is still a drop in a bucket in a massive province of over 8 million residents. And public health officials haven't even told us what percentage of those hospitalizations are patients admitted to hospital for other reasons who just happened to test positive for Covid on a PCR test. In South Africa, 76% of "Covid" hospitalizations are actually incidental, meaning 76% of Covid hospitalizations were actually patients being treated for other conditions who happened to have a positive PCR test while already at hospital.
 |
| Figure 37: Covid hospitalizations and ICU visits in Quebec, Canada, December 22nd, 2021. (Adapted from the Institut national de santé publique du Québec) |
And Quebec's official data now also shows that the majority of Covid hospitalizations (67.6%) and even ICU admissions (69.6%) are in vaccinated people. Some vaccine.
#quebec via @sante_qc for Jan 4, 2022
— Dr° @EzraKahan on Gettr 🇨🇦 🇺🇲 🇦🇹 (@EzraKahan) January 5, 2022
For the first time to majority of patients (69.6%) admitted to the Intensive Care Unit were fully vaccinated. That has been the case for general hospitalizations for a while now. https://t.co/WyeyQgo3ug pic.twitter.com/9qiVUesQUX
The next embedded tweet below shows hospitalization data from Ontario comparing 2020 (light blue) to 2021 (dark blue). Covid-linked hospitalizations are well below levels seen at this time last year. Also, note the benchmark minimum and maximum hospitalization numbers for influenza and pneumonia in prior years (in dashed lines). There has only been a single month (April 2021) when Covid hospitalizations exceeded the normal January peak of influenza and pneumonia hospitalizations seen during the pre-Covid era. During most months Covid hospitalizations have been below the August trough of pre-Covid influenza and pneumonia hospitalizations. Even now, during the massive Omicron wave, hospitalizations in Ontario are dramatically lower than the pre-Covid August trough for influenza and pneumonia hospitalizations.
7. The number of deaths from/with covid-19 in Ontario, 2020-21. pic.twitter.com/su7yRgtIwD
— Milhouse Van Houten (@Milhouse_Van_Ho) December 23, 2021
That's the context you won't hear on the 6 o'clock news. Scary waves on a graph lose their ominous look when there's a bit of context. These hospitalization "waves" are not (and never were) big enough to be considered waves. In the great scheme of things, these hospitalizations are tiny ripples. Hospitals were never at risk of being overwhelmed by Covid. They are being crippled by hysteria and by firing unvaccinated health care workers who are standing up for their individual bodily autonomy, as guaranteed by our Charter of Rights and Freedoms.
And if these hospitalization statistics weren't scandalous enough, Ontario's Chief Medical Officer of Health, Dr. Kieran Moore, has even confirmed that in some hospitals, 50% of Covid hospitalizations aren't actually people in hospital for Covid, they are incidental findings - a positive Covid test in a patient being treated for something else completely unrelated to Covid.
Dr. Kieran Moore admits that COVID hospitalization numbers which were used to justify previous lockdowns are unreliable as 50% were found to be non-covid related in Kingston.pic.twitter.com/hPCr2FnCtf
— CrasHTalk (@CrasTalk) December 31, 2021
Renewed restrictions (including a new curfew in Quebec starting on New Year's Eve) signals that our public health officials know that vaccines have failed (if vaccines worked, why are they imposing curfews and lockdowns on vaccinated people?).
High vaccination rates don't stop the dying. Natural immunity does. And a mild variant like Omicron does. If Germany and Canada had an ounce of sense, they would immediately throw their borders wide open to allow Omicron to spread freely, remove unconstitutional travel restrictions on the vaccinated and the unvaccinated alike, end segregation of unvaccinated citizens, stop fear-inducing PCR tests and border quarantines, and embrace natural immunity.
Instead, they are using coercion to push booster shots in a desperate attempt to double down on a failed strategy in order to avoid admitting the vaccines have failed. Germany is even going as far as to make vaccination compulsory - the ultimate violation of individual autonomy and civil rights. Forced vaccination with a completely pointless vaccine. Germany needs to read its history books a little more carefully.
Failure to let Omicron spread freely in Canada and Germany means they may be condemning themselves to live through another variant (or two or three) before everyone acquires sufficient natural immunity to bring back the flu and relegate Covid to the merry-go-round of endemic cold and flu viruses. Stop listening to public health fearmongering. Stop PCR testing. Live your life. Let 'er rip. Normality is waiting on the other side of a very mild Omicron wave that will do for citizens what the vaccine has failed to do. Most people won't even get symptoms. Even the far more deadly original Wuhan strain caused completely asymptomatic "infections" in 40 to 45% of people. Omicron is as nothingburger as it gets.
Kenya provides several final instructive lessons. In Kenya the flu never went away despite universal mask mandates, social distancing, nighttime curfews, and some short-lived lockdowns, all of which are still in place except the lockdowns. Yet more proof that you can't stop a respiratory virus with masks, nighttime curfews, and social distancing. Check mate, again.
By March of 2021, approximately 61% of Kenyans already had antibodies to SARS-CoV-2... before a single dose of the vaccine had been rolled out! In a country of 54 million people that means that by March of 2021 over 33 million Kenyans had already been exposed to SARS-CoV-2 and had developed antibodies. Yet PCR testing only captured a mere 274,645 PCR "cases" (using December 24th, 2021, numbers), which works out to less than 1% of all infections.
 |
| Figure 38: PCR cases, deaths, and deaths per million in Brazil, USA, South Africa, Sweden, Germany, Canada, India, Kenya, and New Zealand. Adapted from Worldometers.info |
As shown in the chart above, Kenya has one of the lowest death rates of all countries in the world - a mere 96 deaths per million, compared to 788 per million in Canada and 1,314 in Germany. Yet unlike New Zealand, in Kenya the SARS-CoV-2 virus spread so freely that most of their population already has natural immunity.
And, as you can see in the chart below, despite such a vast number of infections, Kenya's experience with Covid was so mild that Covid never even displaced the flu.
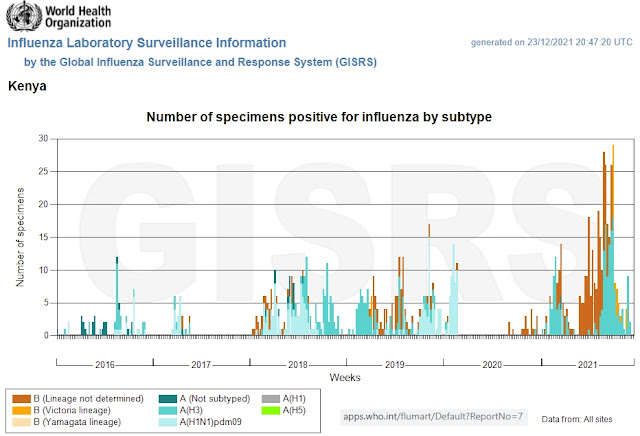 |
| Figure 39: Circulation of influenza viruses in Kenya. The flu never disappeared. The gap starting at the beginning of 2020 is no different than the gap in 2017. (Source: WHO FluNet) |
Kenya's lockdowns and the economic dislocation in the global economy have reversed decades of progress on extreme poverty. Yet by any measure, the Covid virus was all but irrelevant as a medical event. If it wasn't for all the PCR testing, Covid would quietly have coexisted with all the other respiratory viruses, and no-one would have even noticed it was there.
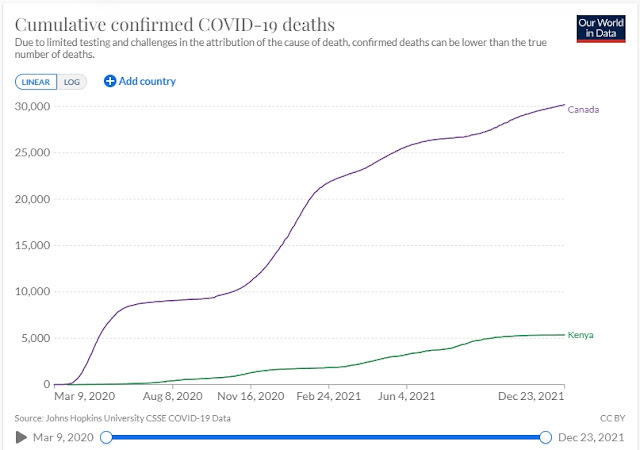
The next chart shows Covid deaths in Kenya, per million, compared to Canada. Rapid spread, vaccination under 10% even today, and yet Kenya only had 1/8th of the death rate seen in Canada.
 |
| Figure 40: Covid deaths in Kenya vs Canada (World in Data) |
Kenya even had roughly the same mix of variants as Canada: the Wuhan strain was followed by Alpha, then Delta, and now Omicron. None were able to displace the flu. Covid was extraordinarily mild in Kenya.
 |
| Figure 41: Variants in Kenya. From CoVariants.org. |
Why did Kenya have a lower death rate despite having such a high infection rate? At 54 million citizens, Kenya's population is 1.4x larger than Canada's. Kenya's population is younger, which undoubtedly played a role both in reducing deaths and in reducing the severity of infections. But on the other hand, 4.9% of Kenya's population is living with HIV (immunocompromised), which is one of the high-risk pre-existing conditions that leads to severe outcomes in Covid patients. That works out to over 2.6 million Kenyans living with HIV compared with only 62,050 Canadians living with HIV. By any measure, Kenya should have been devastated by Covid, but they weren't.
Likewise, obesity is another major risk factor for severe Covid outcomes: in Kenya's tightly packed urban areas over 60% of residents are obese, whereas in rural areas obesity stands at 19.5%. By contrast, in Canada about 26.6% are obese (lower in urban and higher in rural areas). And yet, Kenya's higher vulnerability due to high obesity rates is not reflected in the numbers.
 |
| Figure 42: Cumulative Covid deaths in Kenya vs Canada (World in Data) |
On the other hand, no-one in equatorial Kenya is likely to be vitamin D deficient. Very few people live in nursing homes. Social isolation is rare - elderly citizens typically have lots of community contact. And, as Professor Didier Raoult, director of the Unité de Recherche sur les Maladies Infectieuses et Tropicales Emergentes at Marseilles University in France, pointed out, another of the differences between high income countries (which have all had large death tolls) and low income countries (which have had much lower death tolls), is that public health institutions in high income countries issued mandatory directives requiring all doctors to follow standardized treatment protocols (centrally planned medicine), effectively stripping doctors of their ability to make discretionary decisions in the treatment of their patients. By contrast, in most poor countries the doctor-patient relationship was respected and therefore doctors were able to provide treatment (and preventative care) at their discretion.
As Prof. Raoult said, "It is doctors who should take care of the sick. This cannot be managed with a computer, nor can it be managed with people who make models or mathematics. It's care, okay?", adding that "... each patient has a personal story. You have to see the patient. There are some who are stressed. There are some who are worried. These things reinforce the severity of the disease so they must be addressed. You have to talk to patients, you have to examine them, you have to see if they present particular risks. In other words, you must continue to practice medicine..."
Whatever the precise mix of reasons for Kenya's extraordinarily mild experience with Covid, lifestyle, environment, demographics, treatment strategies, and the doctor-patient relationship all play a role in determining whether a variant causes more or less deaths. If the exact same variant can be significantly milder in Kenya versus in Canada to the point where not a single variant was even able to displace the flu (despite very rapid spread in Kenya), this is clear evidence that the central planning experiment being conducted in Western countries to manage this pandemic is an abject failure.
Why would any country continue push for mass vaccination when vaccines clearly cannot control the pandemic and have a terrible risk profile with many unknown long-term risks even as countries like Kenya, Sweden, Brazil, India, and South Africa have all achieved widespread natural immunity and were done with the pandemic long before their citizens were vaccinated? Why would countries like Kenya still continue their vaccine programs after already having achieved high natural immunity and never having experienced any significant dying from the virus?
For some additional perspective, Kenya has over 3.5 million clinical cases of malaria every single year (in other words, almost 7 million clinical malaria cases in the period covered by the Covid pandemic), whereas Kenya has had only 274,645 PRC-confirmed Covid cases since the start of the pandemic. Malaria is the most common reason for presentation at local hospitals in Kenya, with over 10,700 deaths from malaria every single year. This means Kenya has had approximately 21,400 malaria deaths since the beginning of the Covid pandemic (mostly among young children), which is four times more than the 5,356 Covid-linked deaths over the same period (most Covid deaths were among the very old with severe pre-existing health conditions).
An article in the British Medical Journal has also pointed out this disparity in sub-Saharan Africa, noting that there are approximately 400,000+ malaria deaths per year in sub-Saharan Africa (mostly in children) whereas there were just under 30,000 Covid deaths in sub-Saharan Africa in the first year of the pandemic, two-thirds of which were in just one country (South Africa)). The same article points out that "Aid agencies fear that sub-Saharan African children, the people least likely to be killed by covid-19, will be those most harmed by it in the long term" due to the indirect damage of the pandemic, and that "More than 50 million children lost free meals because of school closures", while "At least 250 million have been pushed out of school, and there is almost no online learning."
[author correction: this article has been updated to remove a reference to Kenya's malaria hospitalization numbers due to a reporting error - a big thank you to one of my readers for spotting it!]
Yet public health authorities in Africa have never imposed lockdowns, mandatory bed nets, nighttime curfews, or mandatory long-sleeved shirts and long pants to stop malaria infections and deaths. Recommendations are made, but no-one is beaten or arrested by a police officer for failing to sleep with a bed net or failing to use mosquito spray. And malaria patients are not forcibly quarantined out of reach of mosquitoes in order to protect other people - we would all recognize that as a clear breach of human rights. Yet all that common sense has been thrown out the window for Covid as public health authorities justify lockdowns, vaccine coercion, civil liberty violations, and massive economic destruction that is tipping countless people in Kenya and all around the world into bankruptcy, joblessness, extreme poverty, and starvation.
On October 7th, 2020, the World Bank stated that as many as 150 million people could be forced into extreme poverty by pandemic management policies. In 2020 alone over 97 million people were already forced into extreme poverty as a result of government management of the pandemic. In Kenya alone, over 2 million people were fell into extreme poverty over the first year of the pandemic - with many now subsisting on only one or two meals per day. And an article by the World Food Program in September of 2020 estimated that "for every COVID-19 death prevented, as many as 80 children may die due to a lack of routine immunizations." To be clear - it's not the virus that did this, it's government intervention in the free choices of its citizens. It's unconscionable. The world has completely lost perspective.
~
The take-home lesson from this deep dive is that lockdowns and vaccines didn't make a shred of difference to Covid outcomes, even as they delayed acquiring natural immunity and caused endless unnecessary misery. Meanwhile, the lifestyle differences that could have dramatically reduced the individual risk of severe outcomes for the vulnerable were completely ignored in favor of a hysterical obsession with vaccines, PCR tests, and suffocating social controls.
Once again, central planning has been exposed as a false god. It's time to stop living in fear; end this authoritarian control over our lives; end the universal vaccine rollout; relegate lockdowns to the dustbin of history; restore individual freedom, rekindle community interaction; get lots of exercise, good food, and sunshine; and live a normal life. At worst, we'll thrive like Sweden. At best, we'll set an example that will spread to other countries to help reverse the misery, starvation, and mental health issues have been imposed on so many people by the government over the course of this central planning experiment. Valuing life begins by respecting the individual autonomy of every single human being.
~
~
If you enjoyed this deep dive, please consider leaving a little something in my Tip Jar to support my independent writing.
And I invite you to subscribe to my free email notifications to receive my latest articles in your inbox. I write about many things, but always with the goal of answering questions essential to science and democracy, and always in the hope of teasing a broader perspective from the mind-numbing noise.
Subscribe for free email notifications for new articles:
COPYRIGHT 2021 JULIUS RUECHEL
This comment has been removed by the author.
ReplyDeleteHas HIV-1 and HIV-2 been isolated and purified? Sauce on this please since you and your wife are experts.
DeleteSo you claim the flu never went away during the last 2 years or what? What is your hypothesis? It was there just before covid arrived and appears now that it becomes endemic.
DeleteThis comment has been removed by the author.
DeleteThis comment has been removed by the author.
DeleteSo flu didnt go away, it was just lost among positive PCR tests - flu symptoms, flu virus but tested positive on Covid, no further test for flu. Right?
DeleteNJP, I am not a research scientist. I am just a retired healthcare professional with a strong interest in what has been happening around this whole pandemic and why. You say(above) that "bad data and wishful thinking" are "quite common in science". You also say that you and your wife did "real science". I guess I am curious as to what you consider to be the difference?
DeleteYou state that Julius' analysis is "pure hogwash" using "worthless data" and that he should have used the animated map from the CDC. Are you aware that the CDC's reputation has been put into question over the last few years (and perhaps longer?). Data collection in the US around SARS-CoV-2 has been considered poor and not reliable. Analysts have been using data from Israel, the UK etc.as a result. Why should the animated map be considered reliable?
I know nothing about the FluChip and VirusChip. You say they were "far superior" to RT-qPCR methods. We know that PCR testing has been fraught with difficulties. Yet the FluChip "landed on the garbage heap of history" because it was not accurate. Am I missing something? How can it be superior if it didn't work?
FYI: I find that I tend to be less trusting when people with strong views and who claim expertise hide behind a pseudonym. This is something you might want to consider going forward.
This comment has been removed by the author.
DeleteThis comment has been removed by the author.
DeleteDear NJP, although I am wondering about some aspect of this article, I am not sure I understood your point. You said flu and cold didn't disappeared. So would you please explain why they are absent of the data? either hospitalisation, records, test or else? My husband and I were wondering about this, so it would be nice of you to explain this, with solid data and real science. By the way, I'm not sure telling others that they don't understand a subject is the best way to convince them you're right. Explaining clearly is easy when you understand well your subject... Or we wouldn't be able to teach high science to students.
DeleteThis comment has been removed by the author.
DeleteHas HIV-1 and HIV-2 been isolated and purified? Sauce on this please since you and your wife are experts.
DeleteYour failure to answer this questions shows a lot about your competence and expertise. Also you writing in awful - logical fallacies abound.
This comment has been removed by the author.
DeleteMore deflection and fallacies. You are a fraud.
DeleteOpinion discarded.
@NJP, I invite you to participate in evidence based discussion, but going forward, I will remove any further posts from you in which you insult readers.
DeleteIf there is something specific you disagree with in my articles, please quote the part you disagree with and provide evidence to support your claim. Credentials and opinions are not a replacement for evidence.
►In regards to your claim that the flu didn’t disappear, the burden of proof is on you to explain the strange phenomena of millions of negative flu tests in thousands of laboratories around the world that demonstrate clearly that flu disappeared. Flu tests continued at similar or higher levels throughout the pandemic, but almost all came back negative. Those are not Covid tests, those are flu tests. Do you have any evidence that those millions of negative flu tests are being faked - because they cannot be turning up negative by accident. It’s the same flu test as before Covid, but now they are finding nothing despite conducting the same number of flu tests. So, the only way to explain away Covid as flu is if thousands of flu testing labs around the world are deliberately faking those results. The burden of proof is on you.
►In regards to your assertion that viral displacement doesn’t exist and that there are no limitations on concurrent infections with multiple viruses… Viral interference was first described in 1929 and there are many decades of literature describing it and researching its origins. And the first interferon (a key component of the innate immune system which contributes to viral interference) was discovered in 1957, and again there is decades worth of research into interferons. If all that research is wrong, it is up to you to provide measurable and testable evidence disproving it - you know well that is how science works. You cannot overturn research with just your opinion and your credentials - you are bound to the same standard of having to provide evidence for your claims.
►As to your claim that shoddy virus sequencing / bad tests are labelling the flu as Covid (ergo, that Covid doesn’t exist), I would like to remind you that Dr. Didier Raoult and his colleagues at the IMU at the University of Marseilles have run thousands of complete DNA sequences on the variants - his lab found and described the very first variant found. We’re not talking about the unreliable PCR tests here (they are clearly a mess) - instead we’re talking full genome sequences in a lab that specialises in tracking this kind of stuff. Dr. Raoult is no lightweight, being the most cited research scientist in Europe in 2014. He has been transparent about all the claims he makes, provides documentation, and has been a fierce critic of the government’s response. Once again, if he is wrong, quote the parts you disagree with and provide evidence of your claims. And if you speak french, I encourage you to watch his latest update: https://youtu.be/_x-eozrCCNM
I don't think that I should discuss science with a specialist on grass-fed cattle.
DeleteThis comment has been removed by the author.
Delete@njp LOL, truly the answer of The Defeated. womp womp
DeleteJust read the ENTIRE article on Sweden cited very early in the article, which proves exactly the opposite of what Julius R. claims, not bothering with the rest of this cherry-picked material.
DeleteWow, your research skills, writing ability (style, tone, diction) and logic are absolutely humbling. Bravo.
ReplyDeleteThank-you Julius for all your hard work in doing this enlightening analysis. But why will most governments (probably) ignore this? Is it just stupidity or something more sinister?
ReplyDeleteThank you Julius, detailed and succinct analysis.
ReplyDeleteThe intelligence in your work shines. I just wish that our medical establishment could see and understand this. We are being led by "leaders" who are just as dumb as those WW1 generals ordering men out of their trenches into withering enemy machine gun fire.
ReplyDeleteThanks
Very thought-provoking as always, Julius. I always look forward to your posts because I learn so much.
ReplyDeleteTwo thoughts: so it is possible to form immunity to an infection that your body successfully fights off without ever developing symptoms? I did not realize that before. Secondly, I wonder if Kenya's lower case rates are partly a result of (perhaps) less testing and the lack of the perverse incentives we have in Canada and US to certify a death as a "covid death" even if the person died of something else and only happened to test positive (or didn't even test positive, if the doctor only thought the person might have covid)?
"...our public health authorities blocked what works (allowing people to lead normal lives) in order to impose a rushed and unproven vaccine experiment on society that does bugger all."
ReplyDelete---Word.
To this point all we know for sure is:
ReplyDelete1) viruses grow beaurocracies.
2) sitting motionless alone indoors is
health.
3) most credentialed homo sapiens are
insane.
Well done, sir.
ReplyDeleteOddly enough, your discussion of Kenya follows on the heels of Bret Weinstein having Gruff Davies and Linda Benskin on his podcast, two experts on vitamin D. One of the big takeaways is that Africa as a whole handled Covid far better than more developed nations and continents, and the guests postulate that it's because people there live a lifestyle that exposes them to far more sunshine, generating much much more vitamin D than we do.
It's well worth a listen, especially while going outside to get some sun.
hydroxychloroquine and Ivermectin as a Zinc Ionophores could be another factor. African population use them as a Sunday drug (prophylactic treatment)
Delete2 questions.
ReplyDeleteCan the PCR test tell the difference between all the different strains apparently in existence.?? What would Kary Mullis say to answer this question ?
In Kenya, is it possible the widespread use of ivermectin contributes to the low rates of the flu ?
thank you.
This comment has been removed by the author.
DeleteDear Julius. Congratulations for your job. I can´t understand why vaccination compete with natural immunity if both, in one way or another, stimulates our immunity system?
ReplyDeleteHi Julius, Thanks for the hard work to expose the fake pandemic and stand for the righteous path we all should strive for.
ReplyDeleteDon't worry about naysayers like the above commentator NJP trying to nitpick points while they fail to produce their own hard and true piece of work.
Interesting analysis that i will have to chew on.
ReplyDeleteI think you should have presented total Covid deaths per population rather than absolute. When you think about Covid as "harvesting" the frail, it did its job in Sweden early on and is still doing its job in Germany, so it does not come as a surprise that deaths in Sweden have subsided but are continuing in Germany (potentially until the same cumulative count per population has been reached - potentially, because there are other virus that can do the harvesting).
The main point I want to make is that, contrary to what you are implying, it may have been smart to delay Covid deaths. Omicron can be thought of as a natural vaccine (whether it is natural remains to be seen), and it seems Canada is reaping the benefit from having delayed the onslaught of Covid for so long. The lesson may be for Germany to cease restrictions now to purge Delta with Omicron and establish natural immunity.
Another point, Delta and previous strains have not only harvested the old and frail but have claimed a great many younger people with no immediately obvious comorbitities, and they have cause damage (long covid) in a great many more.
Like the commentators above, I learn so much from Julius's blogs. Very persuasive analysis of the data.
ReplyDeleteThis comment has been removed by the author.
ReplyDeleteWhy do you remove comments ? Afraid of the other side of debate ?
Deletevery good, in-depth analysis. Two points to consider:
ReplyDelete1) In Kenya (and other developing countries), excess deaths are far higher than official COVID deaths (10x to 100x). Kenya actually has higher excess mortality than Germany or France. Maybe their shocking obesity rate was responsible? https://www.economist.com/graphic-detail/coronavirus-excess-deaths-estimates
2) To say that vaccines had no effect on deaths seems to be too harsh. Alpha and especially Delta would have been much worse without vaccination. Compare western Europe to eastern Europe and Russia. But it is true, vaccines didn't stop the virus, and so the flu couldn't return.
Concerning vaccination/deaths: https://twitter.com/FGarridoB/status/1479826034132402178
DeleteThank you Julius, that's some food for thought as we move forward. It's looking like we'll be seeing peak Omicron by near end of January to early February, especially in parts of Europe, USA, Canada, UK, etc.
ReplyDeleteIf you haven't heard, maybe take a listen to Dr. John Campbell on Youtube. He's a retired nurse teacher and I find his take on the virus to be frank and neither patronizing or panic-mode. He goes through multiple pre-print papers and will always give sensible advice.
Thanks DNR, I will check out Dr. Campbell's videos!
DeleteDecent article thanks. I've been trying to tell people for ages about Viral Interference but seeing what you have presented really confirms it in the case of Covid and Flu
ReplyDeleteThank you for another excellent truth-seeking analysis and for reminding us of the term "old man's friend"--which acknowledges the inescapable reality of human mortality. I remember hearing of a relative who, in old age, referred to death as a friend. Protecting the life and quality of life of old people is very important, but right now the rhetoric of empathy and not overwhelming the hospitals is cynically used to advance an agenda of domination.
ReplyDeleteMuch appreciated Gefen! It is sinister how those who continuously use the rhetoric of empathy have none whatsoever towards anyone who sees the world differently and stands in the way of the utopia they imagine will appear if everyone obeyed their commands. It seems authoritarianism always marches through the front door under a banner of "for your safety."
DeleteVery interesting work to describe natural and adaptive immunity. Your arguments do question the efficacy of vaccines yet I do not see much inquiry on adverse affects of vaccines and vaccine induced deaths, illness. There is plenty of evidence out there showing that connection. Why do you not discuss this?
ReplyDeleteThe evidence on vaccine injuries and deaths is massive indeed. I didn't get into it in this article, but I dealt with in in other pieces, particularly in my deep dive into the probabilites of vaccine injuries and deaths (https://www.juliusruechel.com/2021/06/washingtons-inoculation-gamble.html). The evidence of harm has only gotten much worse since I published that piece. If you're not already following Alex Berenson, @eugyppius, and El Gato Malo, they are doing an amazing job tracking the vaccine issues.
DeleteFirst I congratulate to your work, Julius.
ReplyDeleteI have to state that i miss the comments by User NJP, that were deleted by the author (btw: does that mean NJP or Julius?). Especially one of that comments concerning the question how many unequal parts(sequences) of a region of Genom-RNA of Cov2 are to be expected to exist in one host at one time. In other words, how many variants could be detected normally from one probe if the ask would be to find as much as possible?
the answer should be related to:
"viral interference happens. It also happens between variants of the same virus, as we've witnessed with Covid variants, as new more contagious variants displace older variants causing them to disappear each in their turn, seemingly overnight. An infection with one blocks infection with another."
I understand so far that starting of innate immune reaction wont make it easier for a subsequent/second virus to establish itself. Those mechanism would prefer the earlier one. But isnt enough to explain a complete suppression of all others. As far as i know flu would be the only one virus of many that was gone after Cov2 appeared. Even HCoVs were still there, not diminished.
When Alpha disappeared in Germany, i watched the scene exactly. it looked as Alpha first disappeared, when subsequent Delta comes up. My idea was (and still is) that Alpha has come to its end of evolution, any further mutation would made it unreplicatable. Now we could see the same with Delta.
Genom-Surveillances mentioned rather late the upcomming of Omicron! Where does Omicron suddenly came from? I cant hardly believe that it had been born on just one edge of the globus to immediately start running and conquering so fast all around as it might look like. My imagine is a grade of imperfection in most of the virions that is not negligible. Many virions should contain many different alternative sequences of complete and maybe incomplete Virus-RNA, too.
Many (parts of) hidden variants in each virion or at least in each host as you might say. Could it be possible that those fact(if) wouldnt be detected/discovered by common sequencing-techniques?
My first hope was Julius or NJP could be able to answer, but second i hope for all of you, ladies and gentlemen ;-)
@Udo the commenter NJP removed his own comments on this page. I only removed on comment of his on my "Who Do You Trust If You Can't Trust the Science" article after he launched an unprovoked and extremely rude insult against all the other readers who had left a comment on that article.
DeleteAs to your point about variants burning themselves out, I think so as well - there seems to be many different factors that impact viral displacement, but that is a very big one for why variants burn out.
As to your question aboiut Omicron, I don't know about Omicron's genetic origin, but I do get the sense that the virus can move that quickly around the globe. If you speak French, I suggest following Prof. Didier Raoult, he is constantly providing updates and his institute tracks the dispersal and origins of variants so hopefully he will answer that question soon. I remember him saying that the Marseille 4 variant actually developed in mink (I believe in Denmark) and then made the jump to humans and spread from there. Considering all the possible options presented by the virus hopping back and forth between humans and other animals, like mink and deer, there are a lot of possibilities for where Omicron could have come from.
Udo, I don't think that I should discuss molecular biology, molecular diagnosis, epidemiology, or virology with a specialist on grass-fed cattle.
Deletecheck Campbell on "omicron and mice"
DeleteJulius, greetings from the UK
ReplyDeleteAs I have come to appreciate in reading your website and the Autopsy of a Pandemic book, your analitical and presentational skills have revealed the mechanisms of viral substitution (albeit that we do not necessarily understand all that viruses do) and questioned the polital knee-jerk reactions of those who attempt to govern us.
I really hope that my friends can glean something useful from the implications of your analysis, and move beyond their blinding panic responses that currently are being propagated in the UK.
On a positive note, at last our political classes are beginning to awaken to the foolishness of their responses and pressure is being put on Prime Minister Johnson for a repeal of the Coronavirus Act and a relaxation of the "guidance" regulations regarding the wearing of face masks, etc, etc.
It cannot come too soon!
Thank you for your kind words about my writing and about my book! I too am absolutely estatic about the change of rules in the UK - this will put a great deal of pressure on other jurisdictions to back off.
DeleteThanks for the great article. I'm left with a question about the original sars from 2003-4 and it's return in 2019. Where did it go? What caused sars-cov-1 to morph into sars-cov-2. From personal experience I had a severe respiratory virus/flu(?) in October of 2017.
ReplyDeleteIt was unlike anything I've had previous. It was like breathing through a pin hole and the inside of my nostrils had raised wave pattern projecting inward that was hard like bone yet looked like flesh which went back to normal as I healed. I remember the date because it was my brother's birthday and he had phoned on that day to ask how our 'flu's' were, and he passed away that Christmas from an oxycodone overdose. We talked about the last time we had talked, which was when we were sick in October, so I'm very sure of the date.
So my question is, what happened to sars, where did it go after 2003? Has it been there the whole time transforming itself, and why did it reappear in 2019? Did I have it in 2017?
Excellent article
ReplyDeleteI really enjoyed this article.
ReplyDeleteIt seems to me then from what you are saying here, that if you take a country to like Sweden (and to some extent the UK) where I live, there is evidence that far more people had got Convid (and recovered) than was known. (This also means the infection fatality rates would have been much lower than is normally assumed). (And this high level of exposure can be evidenced from antibody tests)
It is also abundantly clear (as you explain in this piece) that there will have been a lot of prior infection and recovery in places like Africa too.
The key question all these experimental injection fans should be asking themselves is this: If the quackcines were so important in "defeating Convid", then where are all the bodies in Africa, where they have such a low rate of quackcination?
Here in England and in Sweden and just about everywhere else (because of this barmy Big Pharma - Great Reset Alliance) the story being told is "It is the vaccines wot won it" whereas it was really exposure, naturally acquired herd immunity and a much wider immunity than they admitted that did it. In other words, their narrative is a lie - and is simply designed to set us up for more of these failed injections in the future for other diseases, which our bodies could easily deal with naturally.
What I would like to see if a table of each country with two columns.
In column one is % of the country that has had the quackcine ordered from highest to lowest.
Against that, in column 2, is the excess death rate compared to normal for that country, (perhaps with some comment non average age, given that is the biggest factor driving death rates from Convid).
Anyone know if any such up to date tables exist?
I think that would nail the lie that the damn quackcine for Convid does not work - and we have been lied to.
It is clear NJP did not read the article and was merely triggered by the title, or at best grazed over a paragraph or two. The author provided clear in depth answers to your questions in the section, which were already clearly explained in the article.
ReplyDeleteTwo weeks later, and Sweden's covid death rate is no longer flat.
ReplyDeletehttps://ourworldindata.org/covid-deaths
Yeah it already "lost" my comment, after I highlighted and cut-and-pasted and then cited the same linkused in the article about Sweden, which of course DID deploy masking, social-distancing, and much more to fight both COVID and the flu, all of it based in a single payer, centrally planned health care system as well!
ReplyDeleteThis is the first of your articles I've read and I really enjoyed it. I also learnt a lot! We'll done. It's been clear to me that most the developed world has been on the wrong path in trying to tackle Covid and this article clearly lays that out. I'm in New Zealand and it's going to be a very interesting few months here as the government, and 70% of people who only read corporate media, start to panic as cases and likely hospitalisations rise.
ReplyDeleteGreat read, but I have one question: How do you "justify" or explain the high excess mortality rate in almost all countries that were hit by covid?
ReplyDeleteSuperbe article, the best I have read so far about the covid pandemic! I will do my best to promote it!
ReplyDeleteI live in an area that got hit hard early by the virus. My ballpark estimation is that 1 in 50 who were sick or heavily exposed actually got tested. But, media brainwashed hypochondriacs - usually pretty nutty people - who were never exposed would get tested many times a month. It was so obvious that the testing data was absolute garbage and that's not factoring in the problems with the PCR test itself.
ReplyDeleteEveryone in my area with a smidgen of common sense figured the good, the bad, and the ugly about this virus early on based on their experiences with the virus. Albeit, with zero assistance from those whose job it is to help.
When experts and authorities are going off of data that is so obviously bad based on the observations in your personal life eventually you just ignore everything they say.
Its going to take at least a generation for the scientific and bureaucratic class to recover their reputations. I'm highly educated and used to hold these types of people in high regard. I respected them immensely.
But now, I viscerally hate them.
There needs to be trials and long imprisonments for the pain and suffering these people have caused society.
I see, Julius is just a "specialist on grass-fed cattle". What can he know about viral infections and data science? Reminds me of that Albert Einstein, he was just a Patent Clerk. What could he know about space and time and gravity and radiation and atoms?
ReplyDeleteEinstein's educational background and the zeitgeist in physics were formidable factors in the 1905 publication that launched him onto the world stage. Julius Reuchel is and will remain an obscure conspiracy theorist, but apart from that, sure, it's a valid comparison!
DeleteThere are conspiracies. J S Bach was an organist & Court servant, obscure for a long time - so you never know.
DeleteOf course "there are conspiracies," for example, you can find a host of carefully written scholarly articles at the kennedysandking dot com website, but Reuchel's material will simply languish in obscurity because it cannot survive criticism via a publication in peer-reviewed scientific journals. If it could do so, or if these baseless arguments had any substance, in other words, Reuchel would be a serious candidate for the Nobel Prize in Medicine, and I would be one of tens of thousands if not tens of millions of interested observers relentlessly advocating his articles, books, website, the works!
DeleteDon't shoot the messenger. If you have a specific argument against it, make it and we will all learn something.
DeleteAgainst what, specifically? This is an amorphous mass of inchoate claims about vaccines, masking , social distancing and how diseases spread, but absolutely no clear way forward is offered as a subsitute, and there is no credible, cogent, lucid argument at all based on facts that show the vaccines, masking, and social distancing are ineffective. There is a surfeit of charts and data points, but nothing you could expect to survive an attempt to get it published in Scientific American, Nature, The New England Journal of Medicine, or some specialist medical journal and virology. "Extraordinary claims require extraordinary proof," and if this allegedly world-shaking set of superb insights is really so monumentally important, where's the attempt by Reuchel to do any of that? Where is his folder of rejection letters from the big bad science experts conspiring to keep his genius-inspired discoveries from the world? I suggest that folder does not exist, because Reuchel knows very well he has no case to make, but he can make money in the meantime claiming he is in possession of vital, revolutionary understandings unfairly shut down by The Powers That Be. This particular style of hoaxing is not new at all, it's tedious and predictable. I only ended up here on a friend's recommendation that it was interesting and unusual, but it's neither, really.
DeleteYou made a mistake attacking Julius in this manner. He is a master of quotes suffering from a severe case of Blogitis. Alex Berenson, a successful writer of crime stories, suffers from the same disease. Alex and Julius love to quote from the NEW SCIENCE "results" on variants, virus evolution, and viral interference. Mind you, some basic knowledge of molecular epidemiology would be required to understand the failures of such narrative.
DeleteThat isn't at all clear - the onus probandi is not on me, it is completely on Julius, like anyone else, to vindicate his putatively correct and important theories in, for example, a specialist medical journal on virology or biomedical epidemiology. As it is, my "mistake" is only in taking this obscure blogger seriously enough to post comments in between poring overthe play Macbeth, to verify my own observations about what I think are crucial aesthetic lacunae in Joel Coen's current film starring Denzel Washington and Fraces McDormand, The Tragedy of Macbeth. There will still be a vigorous and exciting discussion of Macbeth and Shakespeare's other dramas in a few years, when this particular article and blogger remain mired in Dunning-Kruger obscurity. That's my view, so sue me!
DeleteNJP's profile reminds me of the "Hunting of the Snark".
ReplyDeleteHe had bought a large map representing the sea,
Without the least vestige of land:
And the crew were much pleased when they found it to be
A map they could all understand.
"What's the good of Mercator's North Poles and Equators,
Tropics, Zones, and Meridian Lines?"
So the Bellman would cry: and the crew would reply
"They are merely conventional signs!
"Other maps are such shapes, with their islands and capes!
But we've got our brave Captain to thank
(So the crew would protest) "that he's bought us the best—
A perfect and absolute blank!"
Hey Julius, pay no attention to the trolls - I find your analyses interesting, enlightening, and useful, as do so many other people. Don't ever give up writing.
ReplyDeleteHey I hope he writes endlessly, it keeps him out of trouble and he enjoys piling on the bilge, so why not?
DeleteChacun a son gout!
This article is so much more elucidating than any news outlet, CDC or NIH, and Andrew Kaufman. This is very good stuff, you and Chris Martenson are great
ReplyDeleteYou need to at least attempt to master the main outlines of the so-called "conventional view" on this before deciding he is on to some devastatingly brilliant "outlier" theory of misunderstood genius, those claims are so routine in every possible field of science the list is practically endless.
ReplyDeleteYes, I had this shoved under my nose, under a throwaway Tweet of mine on a somewhat different topic, but kept shaking my head. Can't see viral interference being a significant mode of variant replacement myself. It would require the variants to continually be dual-infecting people, with the new variant always getting there first, rather than picking off the susceptible differentially. It'll happen from time to time, but why ignore differentials in R? The bulk of contests taking place within individuals, rather than within populations as more conventionally viewed? Highly unlikely.
DeletePray for us in NZ
ReplyDeleteJulius,
ReplyDeleteMany thanks for your enlightening analysis/breakdown of this topic!
With regard to omicron and increasing death rates (i.e. Brazil => see ourworldindata). What are your thoughts? Is this OAS? Multiple factors at play?
Richard
Hi Julius, 5 months later (and a couple of dollar short) somebody is asking the same question: https://news.google.com/articles/CAIiEN3MvF3ZdsyuTrDfhlMucxoqGQgEKhAIACoHCAowqeP_CjDdg_oCMMTh6QU?hl=en-CA&gl=CA&ceid=CA%3Aen
ReplyDeleteYou may want to spell it out for them.
I'm wondering whether Malaria is displacing Covid in Sub Saharan countries, just as Covid displaces the flu.
ReplyDeleteI don;t buy into the Ivermectin argument, because I know very few Africans who take this regularly.
Thanks for the post
ReplyDelete